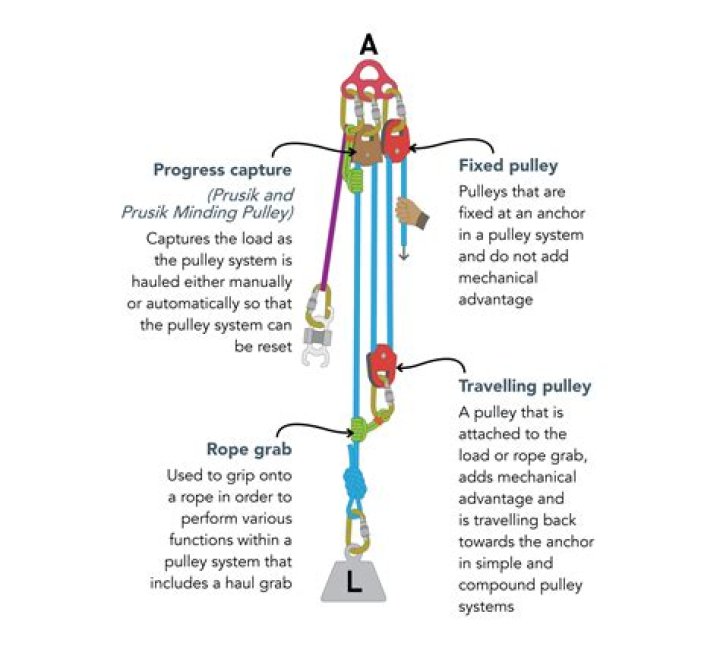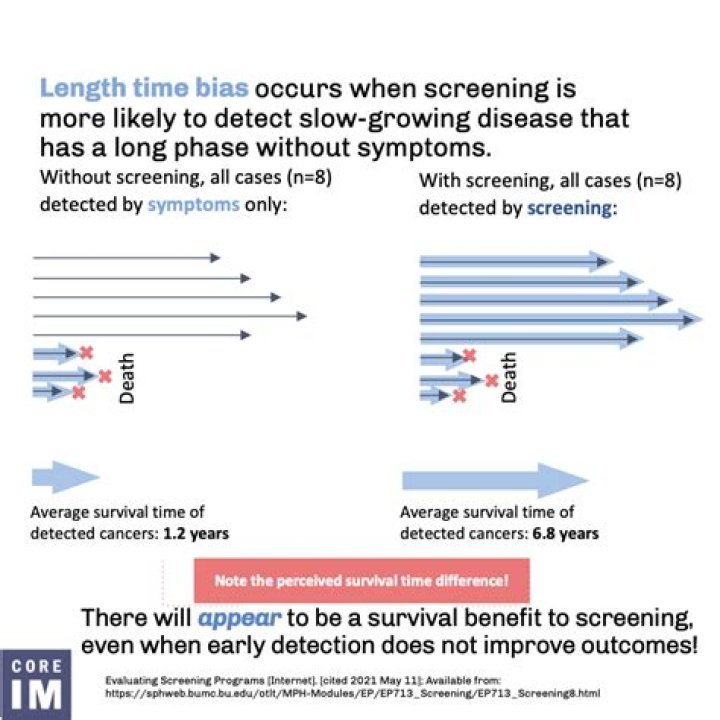
Length time bias (or length bias) is an overestimation of survival duration due to the relative excess of cases detected that are asymptomatically slowly progressing, while fast progressing cases are detected after giving symptoms.
What is lead time bias in screening?
Lead-time bias occurs when a disease is detected by a screening or surveillance test at an earlier time point than it would have been if it had been diagnosed by its clinical appearance; this time lag or “lead time” during which the disease is asymptomatic is not taken into account during the survival analysis (Figure …
What is lead time bias example?
Lead time bias refers to the phenomenon where early diagnosis of a disease falsely makes it look like people are surviving longer. This occurs most frequently in the context of screening. For example, a man with metastatic lung cancer dies at age 70. His cancer was discovered 1 year ago, when he was 69.
How much difference does early screening and detection make to breast cancer survival rates?
Women whose breast cancer is detected at an early stage have a 93 percent or higher survival rate in the first five years. So the Carol Milgard Breast Center and TRA-MINW advise women to get screening mammograms every year starting at age 40.
How do you get rid of time bias length?
How to Avoid Bias
- For length time bias – count all outcomes regardless of method of detection.
- For volunteer bias – count all outcomes regardless of group; follow-up those who refuse to get outcomes.
What is late Look bias?
Late Look Bias | occurs when the data is gathered or analyzed at an inappropriate time. Lead-time Bias | occurs when one test detects disease earlier so there seems to be increased survival. Publication Bias | occurs when only positive or favorable results are published.
How do you fix lead time bias?
For lead time bias – use mortality rather than survival rates. A randomized clinical trial design can reduce biases: For length time bias – count all outcomes regardless of method of detection. For volunteer bias – count all outcomes regardless of group; follow-up those who refuse to get outcomes.
Why are breast exams no longer recommended?
Breast self-examination is not recommended in average-risk women because there is a risk of harm from false-positive test results and a lack of evidence of benefit. Average-risk women should be counseled about breast self-awareness and encouraged to notify their health care provider if they experience a change.
What is the difference between lead-time bias and length bias?
Lead-time bias: Overestimation of survival duration due to earlier detection by screening than clinical presentation. Length-time bias: Overestimation of survival duration due to the relative excess of cases detected that are slowly progressing.
What is procedure bias?
Procedural bias is where an unfair amount of pressure is applied to the subjects, forcing them to complete their responses quickly. For example, employees asked to fill out a questionnaire during their break period are likely to rush, rather than reading the questions properly.
Does screening mammography reduce breast cancer–specific mortality?
Randomized controlled trials (RCTs) initiated 50 years ago provide evidence that screening mammography reduces breast cancer–specific mortality for women aged 60 to 69 years (solid evidence) and women aged 50 to 59 years (fair evidence).
What are the benefits of mammography for women aged 40-49 years?
The benefit of mammography for women aged 40 to 49 years is uncertain. [ 1, 2] There are randomized trials in India, Iran, and Egypt that have studied the use of clinical breast examination (CBE) as a screening test.
What is the most widely used screening modality for breast cancer?
Note: Separate PDQ summaries on Breast Cancer Prevention, Breast Cancer Treatment (Adult), Male Breast Cancer Treatment, and Breast Cancer Treatment During Pregnancy are also available. Mammography is the most widely used screening modality for the detection of breast cancer.
What is the prevalence of false positive breast cancer screening tests?
Magnitude of Effect: Specificity in women aged 50 to 59 years was 88% to 99%, yielding a false-positive rate of 1% to 12% for all women screened. [ 23] Study Design: Descriptive, population based. Internal Validity, Consistency, and External Validity: Good. False Negatives with Potential False Reassurance and Delay in Cancer Diagnosis.