This includes assessment of skin color, moisture, temperature, texture, mobility and turgor, and skin lesions. Inspect and palpate the fingernails and toenails, noting their color and shape and whether any lesions are present.
How do you document skin turgor in nursing?
To check for skin turgor, gently grasp skin on the patient’s lower arm between two fingers so that it is tented upwards, and then release. Skin with normal turgor snaps rapidly back to its normal position, but skin with poor turgor takes additional time to return to its normal position.
How do you inspect skin?
Inspect and palpate skin for the following:
- Color: Contrast with color of mucous membrane.
- Texture.
- Turgor: Lift a fold of skin and note the ease with which it moves (mobility) and the speed with which it returns into place.
- Moisture.
- Pigmentation.
- Lesions.
- Hair distribution.
- Warmth: Feel with back of your hand.
How would you describe skin turgor in nursing assessment?
Skin turgor refers to the elasticity of your skin. When you pinch the skin on your arm, for example, it should spring back into place with a second or two. Having poor skin turgor means it takes longer for your skin to return to its usual position. It’s often used as a way to check for dehydration.
Why do nurses do a skin assessment?
To identify patients at risk for skin failure, assessment should be conducted on admission to the ward to identify any issues with the skin’s integrity such as existing wounds (especially pressure injuries) or vulnerable pressure points, excoriation and rashes.
Why is skin assessment important in nursing?
A clinical assessment of the skin by a healthcare professional, taking into account any pain reported by the person, may predict the development of a pressure ulcer. The results of the skin assessment can be used to offer suitable preventative interventions to people who are at high risk of developing pressure ulcers.
Why do we do skin assessments?
A thorough skin assessment gives you important information about potentially serious diseases, especially in older adults who are vulnerable to skin breakdown.
What 4 things should you examine the skin during palpation of the skin?
Inspect for lesions, bruising, and rashes. Palpate skin for temperature, moisture, and texture.
Why is a skin assessment important?
As discussed above, one purpose of comprehensive skin assessment is to identify visible changes in the skin that indicate increased risk for pressure ulcer development. However, factors other than skin changes must be assessed to identify patients at risk for pressure ulcers.
What is a comprehensive skin assessment?
Comprehensive skin assessment. In the healthcare setting, a comprehensive skin assessment is a process in which the entire skin of a patient is examined for abnormalities. It requires looking at and touching the skin from head to toe, with a particular emphasis on bony prominences and skin folds.
What is a nursing assessment tool?
Nursing assessment is one of the health diagnostic tools used for assessing the nursing care implemented by a particular health care organization to its patients. Such kind of appraisal document seeks for direct interaction of the nurses with the patients so that it helps in ensuring better nursing care plan in future.
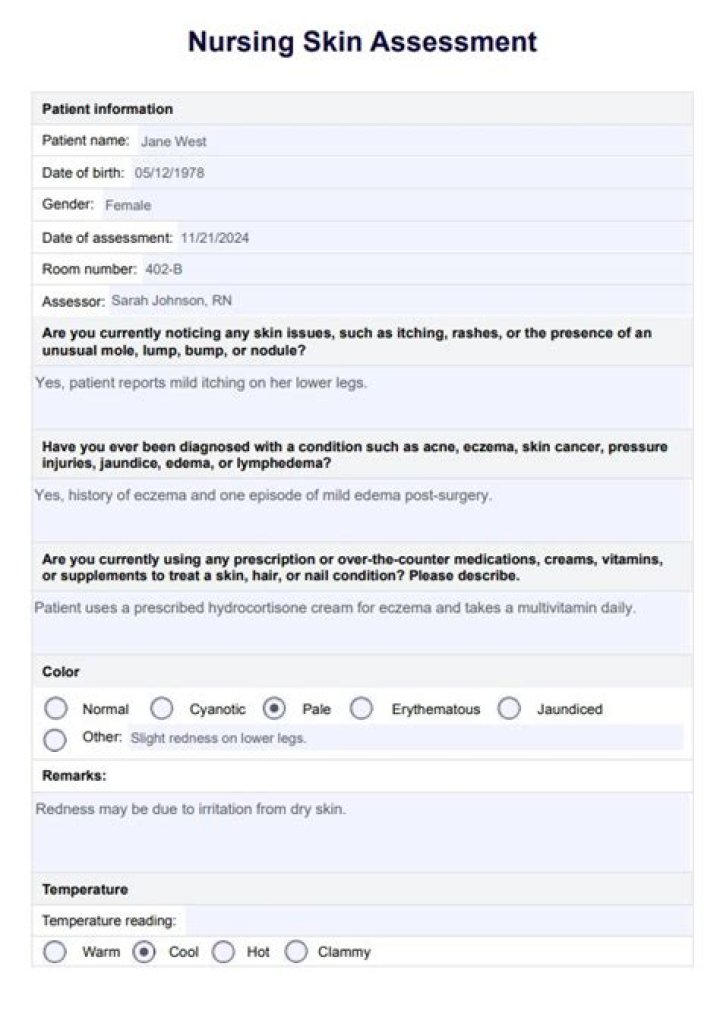
What is medical assessment form?
Printable Patient Assessment Form. The patient assessment forms are used in health centers and hospitals to document the assessment results of the physical examination and medical tests carried out on a patient. The patient assessment form is mandatory document which must be filled by the doctor or medical practitioner attending a patient.